

Cleaning is intended to remove soils (e.g., patient secretion, tissues and inorganic material such as salts) from surfaces of reusable medical devices (RMD). Although cleaning takes place after point of use processing, patient secretions, tissues and inorganic material such as salt may remain on RMD surfaces. They could interfere with sterilizing or disinfecting agent or generate endotoxin or pyrogen risks
Disinfection, is intended to reduce the microbial load. Disinfection may be the last step before use of an RMD or take place in preparation for sterilization.
- Before sterilization, disinfection improves the preparation of a RMD for sterilization. It may be required or recommended in some countries as an occupational health and safety measure for operators in charge of packaging.
- As the last step before use of an RMD, the objective of disinfection is to render the RMD safe for the patient according to Spaulding classification principles.
![]() Although cleaning and disinfection are different in practice, they are often grouped in a cleaning and disinfection process (e.g., automated washer disinfector). Therefore they were grouped together in a single chapter of these guidelines
Although cleaning and disinfection are different in practice, they are often grouped in a cleaning and disinfection process (e.g., automated washer disinfector). Therefore they were grouped together in a single chapter of these guidelines
Most detergent formulations include a surfactant, which reduces the surface tension of water thus easing the wetting of surface and breaking up of soils). Other components of detergents are buffers which improve the compatibility with RMD material and softeners which reduce the potential negative effect of hard water (spotting and deposit on surface).
|
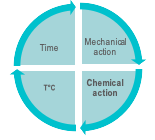
The 4 conditions for efficient washing are illustrated by the Sinner circle. 1. Mechanical action by manual brushing, flushing, swabbing or wiping, automated spraying or flushing, cavitation (in ultrasonic cleaner). 2. Chemical action of cleaning agents that decompose protein, lipids and ease the removal of soils from surfaces 3. Contact time of all RMD surfaces with the cleaning agent and water solution. 4. Temperature of the cleaning solution. Concentration, exposure time or temperature exceeding the instructions of the cleaning agent manufacturer may present a risk for operators, damage an RMD, and do not mean greater cleaning efficacy.
|  |
Rinsing with adequate water quality (water hardness, pH and temperature) removes chemical agent residues. Rinsing after disinfection is often called final rinsing to differentiate it from intermediary rinsing which takes place after cleaning. Drying with adequate air quality removes residual humidity which favors recontamination and impairs sterilization. In some countries, alcohol rinsing is used to accelerate drying (specifically for GI endoscope reprocessing). This practice is not allowed in Europe and some other countries due to fixative properties of alcohol.
Lubrication is implemented when specified in an RMD manufacturer's IFU. Lubricants are intended to protect against friction on the surfaces of an RMD. RMD manufacturer's IFU's specify the type of lubricant to be used and which parts of an RMD requiring lubrication. Non-approved lubricants can interfere with sterilization or disinfection, create harmful by-products, and/or damage the device or the sterilizer/disinfection equipment. Water soluble lubricants are commonly preferred. |
- Thermal disinfection is performed in automated washer-disinfectors (WD) with hot water at specified temperature. Thermal disinfection is commonly used for surgical instruments intended for steam sterilization. Lubrication is applied as recommended by RMD manufacturer IFU.
Reusable containers and other heat and moisture compatible items are also typically thermally disinfected. WD disinfection and rinsing are combined in thermal disinfection. Thermal disinfection provides good drying. A rinse aid may be added to the rinse water. Thermal disinfection is also efficient for self-disinfection of the washer-disinfector.
![]() Manufacturers of thermal WD may however offer or recommend periodic self-disinfection cycles
Manufacturers of thermal WD may however offer or recommend periodic self-disinfection cycles
The improvement of lethality with hot water temperature can be predicted. For instance, for heat resistant microorganisms, 10 minutes at 80°C has the same lethality effect as 1 minute at 90°C or 100 minutes at 70°C. By convention the time (expressed in second) to obtain a given log reduction at 80°C serves as a reference and called A0 for heat resistance microorganisms. In the previous example A0 equals 600 s (10 minutes at 80°C). Higher A0 means longer exposure time at 80°C or shorter time at higher temperature according to the A0 equation.
See annex B of international standard ISO 15883-1 for more information. Local regulation, recommendations or habits define the A0 thresholds according to the level of contamination of an RMD and its intended use. A0 of 60 s is commonly recognized as the minimum to be targeted for low risk items according to Spaulding classification principles. 600 s is the minimum for other items. Automated WD for surgical instruments complying to ISO 15883-2 must have one cycle with an A0 value above 3000 (e.g. a value of 50 minutes at 80°C or practically 5 minutes at 90 °C or 2 min and 30 s at 93 °C). A0 values of 3000 or above are recommended in some countries. Others consider 600 s as sufficient for most items (considering that thermal disinfection always takes place after cleaning and that residual spores (if any) will be eradicated by sterilization
|
Tests are performed with microorganisms known for their high resistance to the sterilization process (usually bacterial spores).
Once the process has been characterized, it must be verified that an RMD can be efficiently sterilized. The 106 inoculum is placed at the position determined as the most difficult to sterilize on or within an RMD. RMD's are packaged and inserted in a representative challenging load. For routine controls, inoculums may be placed in process challenge devices (PCD) |  |
When allowed according to the IFU of an RMD manufacturer IFU, automated cleaning and disinfection processes (WD and AER) are preferred over manual processes.
Washer-disinfector (WD) and automated endoscope reprocessors (AER) are more reproducible (less human dependent), safer for operators (reduction of exposure to chemicals, aerosols, handling risk) and provide automatic recording.
For the cleaning and disinfection of RMD in preparation for steam sterilization International standards express a preference for thermal disinfection
![]() ISO 15883-12 says: Thermal disinfection processes are more easily controlled and avoid the hazards to staff, patients and the environment that can occur through the use of chemical disinfectants. “Thermal disinfection is efficient to eliminate most microorganisms (except spores) and provide good rinsing and drying”.
ISO 15883-12 says: Thermal disinfection processes are more easily controlled and avoid the hazards to staff, patients and the environment that can occur through the use of chemical disinfectants. “Thermal disinfection is efficient to eliminate most microorganisms (except spores) and provide good rinsing and drying”.
Manual or ultrasonic pre-cleaning may be required before automated cleaning and disinfection of complex and/or heavily soiled RMD.
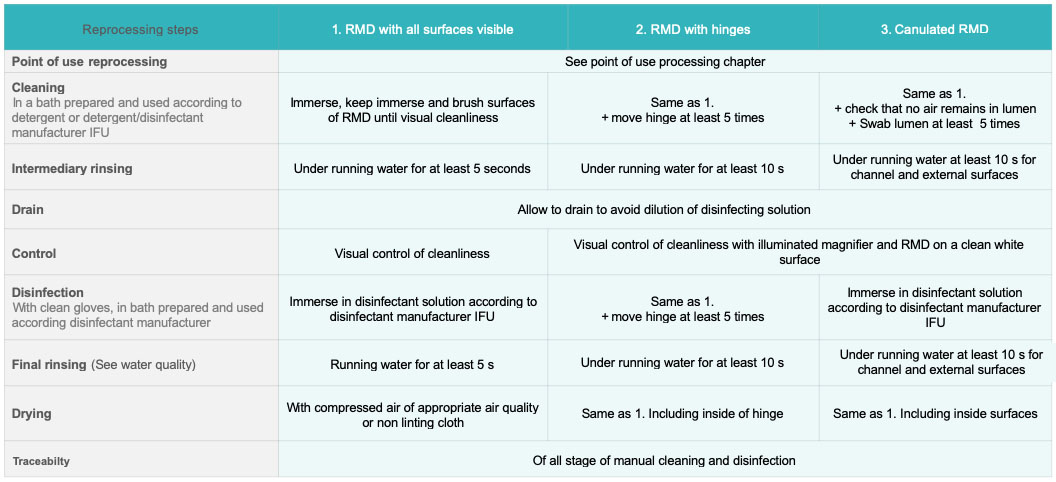
Manual wiping is used when immersion in bath is not allowed by RMD manufacturer IFU
![]() International standard ISO 176648says :
International standard ISO 176648says :
At least one validated automated cleaning method (which may include a validated manual pre-cleaning method) shall be specified unless the medical device cannot withstand any such process, in which case a statement shall be provided which alerts the user to this issue. A validated method of manual cleaning shall be specified if automated cleaning is not possible.
if the medical device is intended to be disinfected, at least one validated automated disinfection method shall be specified unless the medical device cannot withstand any such process, in which case a statement shall be provided which alerts the user to this issue. If the medical device is intended to be disinfected, a validated method of manual disinfection shall be specified if automated disinfection is not possible
 |
Principles for bath preparation, loading and unloading are as follows
- Follow the instructions of ultrasonic cleaner and detergent manufacturers for dosing and temperature of bath. The water temperature is between 27 °C (80 F) and 43 °C (109 F) and never above 60 °C (140 F) because most proteins denaturate above that temperature. For ultrasonic systems without thermoregulation room temperature might be preferable as energy delivered by the ultrasonics wave will increase the temperature of the bath.
- The bath is degassed at each filling. This is done by filling the unit, closing the lid and running a cycle for 5 to 10 minutes
- RDM are placed in a tray (never directly on the tank end) and open wide, not superimposed to avoid shadowing. When applicable, connect lumen devices to flushing ports. If other specific positioning accessories and features are used, refer to the manufacturer’s IFU.
- The cavitation process may create aerosols, so the ultrasonic bath should have a lid that must remain closed during the cleaning process.
- The process time is per the manufacturer recommendations (usually between 5 and 10 minutes)
- If rinsing is not performed by the ultrasonic cleaner, the RMD is rinsed and dried manually
The bath is preferably changed after each use (i.e. after reprocessing cycle). Ultrasonic cleaning equipment is cleaned every day that it is used and according to manufacturer IFU. Local recommendations specify that it has to be refilled after each use or daily and each time the bath is visibly soiled.
![]() National regulation or recommendations may forbid the use of ultrasonic cleaners if a prion risk has been identifiedMD
National regulation or recommendations may forbid the use of ultrasonic cleaners if a prion risk has been identifiedMD
Washer-Disinfectors spray or flush pressurized water mixed with a detergent on surfaces of RMD and lumen. The cleaning stage is followed by a thermal or chemical disinfection.
Various types of WD are:
- Washer-disinfectors with a thermal or chemical disinfection stage for surgical instruments; these are available in different configurations, e.g. single chamber (pass-through or single door) or multi-chamber versions.
- Cart washers for carts, reusable containers, surgical basins and other non-invasive , non-critical medical devices; these can be single or multi chamber (steps of the cleaning and disinfection process are performed in different chambers).
- A table top washer-disinfector for dental handpieces and turbines.
![]() Automated endoscope reprocessor AER are described separately in automated endoscope reprocess (AER) paragraph
Automated endoscope reprocessor AER are described separately in automated endoscope reprocess (AER) paragraph
Except for table top washer-disinfector for dental handpieces, WD’s are covered by international standards
![]() International Standard ISO 15883 includes general requirements ISO 15883-1 and specific parts dedicated to each type of WD;
International Standard ISO 15883 includes general requirements ISO 15883-1 and specific parts dedicated to each type of WD;
1![]() Compliance to ISO 15883-11 and subsequent parts2,3,4,5,6,7 may be required (for instance in Western Europe)
Compliance to ISO 15883-11 and subsequent parts2,3,4,5,6,7 may be required (for instance in Western Europe)

WFHSS key recommendations for cleaning & disinfection
Cleaning & disinfection before use or in preparation for sterilization
Go to Objective of cleaning & disinfection →
1 of 12 Clean, dry, disinfected RMDRMD ready for use or ready for sterilization
Go to Objective of cleaning & disinfection →
2 of 12 PrecleaningManual precleaning for flexible scope
Go to Automated endoscope reprocessing (AER) →
Ultrasonic cleaning if allowed by RMD manufacturer IFU
Go to Ultrasonic cleaning →
AER for flexible GI scopes
Go to Automated endoscope reprocessing (AER) →
WD for surgical instruments
Go to Washer Disinfector (WD) →
4 of 12 Manual cleaning and disinfectionWith cleaning and disinfection solution
Go to manual cleaning and disinfection →
5 of 12 Manual disinfectionWith disinfection solution
Go to manual cleaning&disinfection →
6 of 12 Manual cleaningWith cleaning & disinfection solution
Go to manual cleaning&disinfection →
7 of 12Automated processes unless not allowed by RMD manufacturer IFU
Validated cleaning & disinfection process
Go to ![]() WFHSS recommendations for cleaning and disinfection →
WFHSS recommendations for cleaning and disinfection →
As needed, precleaning for complex and heavily soiled RMD and for flexible scopes
9 of 12RMD visibly clean and dry
Control of process parameters for AER and WD
Go to cleaning & disinfection and quality →
10 of 12According to SOP combined or
sequential cleaning & disinfection
Go to manual cleaning&disinfection →
11 of 12Thorough and consisten cleaning,
repeat if visible soil
Go to ![]() WFHSS recommendations for cleaning & disinfection →
WFHSS recommendations for cleaning & disinfection →